IAN LAVERY MP says an immediate focus on raising wages and reducing costs must be part of a strategy to show Labour can deliver for workers again

Potential for HIV cure beyond the state of the ART?
Medicine has long been able to guarantee HIV patients an almost normal life and now it can fully cure the virus too — but the treatment is not appropriate for all, explain ROX MIDDLETON, LIAM SHAW and JOEL HELLEWELL
Friedrich Merz’s call for a new Plaza Accord ignores how Washington’s 1985 currency ambush destroyed Japan without fixing US deficits — China, a sovereign socialist state with 1.4 billion consumers, cannot be bullied the same way, writes CARLOS MARTINEZ
World Peace Council president PALLAB SENGUPTA assesses the challenges facing the international peace movement and sends greetings to the Liberation AGM
KIERA MARSHALL says there is a gulf between the privileged circles in which most politicians move and the lives of working-class youth in left-behind estates – and as a newly elected Senedd member she’s determined to do something about it
ANGUS REID and ANDREW JOHNSTONE report on an initiative that we must take this summer
At last weekend’s International Conference Against War, LINDA PENTZ GUNTER talks to the Palestinian physician and politician about the struggles ahead to achieve a truly free Palestine






THE development of antiretroviral therapies (ART) has meant that, where available, people living with the human immunodeficiency virus (HIV) now have a normal life expectancy.
Yet despite this achievement, ART is not a cure for HIV and people living with HIV need to keep taking ART for the rest of their life to prevent the development of acquired immune deficiency syndrome (Aids).
As of this moment, two people have been — or at least appear to have been — completely cured of HIV infection, the virus was eradicated from their body and they no longer needed to take ART.

Similar stories
RICHARD SHILLCOCK examines an enjoyable, but philosophically conventional book, and urges Marxists to employ their capacity to embrace the totality in any explanation
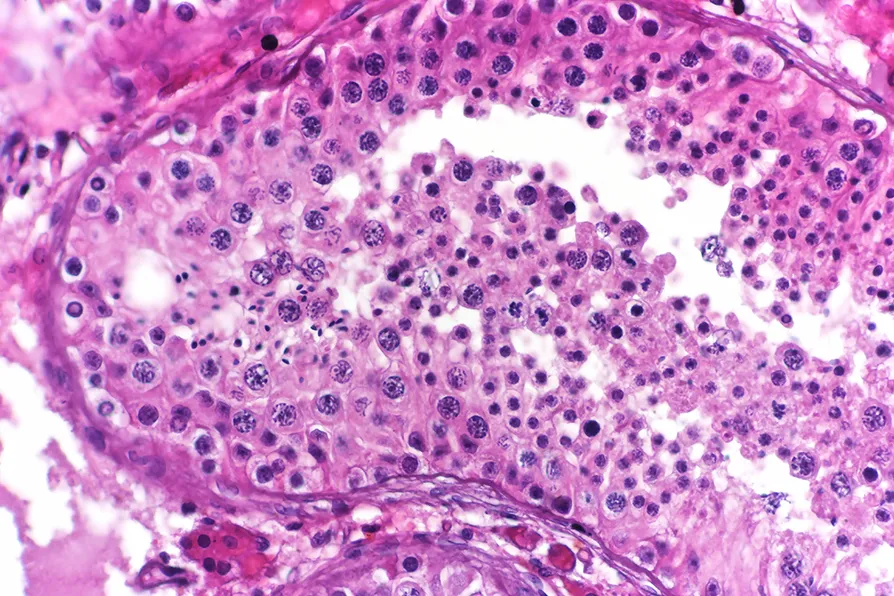
New research into mutations in sperm helps us better understand why they occur, while debunking a few myths in the process, write ROX MIDDLETON, LIAM SHAW and MIRIAM GAUNTLETT

Olive oil remains a vital foundation of food, agriculture and society, storing power in the bonds of solidarity. Though Palestinians are under attack, they continue to press forward write ROX MIDDLETON, LIAM SHAW and MIRIAM GAUNTLETT