MBDA’s Alabama factory makes components for Boeing’s GBU-39 bombs used to kill civilians in Gaza. Its profits flow through Stevenage to Paris — and it is one of the British government’s favourite firms, reveals SOLOMON HUGHES


Public pharma v abusive prices: the case of the latest HIV-prevention drug
ALAN ROSSI SILVA argues that Gilead’s HIV prevention drug, while promising, highlights systemic failures in the pharmaceutical industry, showing the need to shift towards state-owned drug development and production

President Maduro mobilises the 4.5 million-strong Bolivarian National Militia in response to US ‘threats’, vowing to defend the country’s sovereignty and independence, DEVIN B MARTINEZ reports
Washington plays innocent bystander while pouring weapons and intelligence into Ukraine, just as it enables the Gaza genocide — but every US escalation leaves Ukraine weaker than the neutrality deal rejected in 2022, argue MEDEA BENJAMIN and NICOLAS JS DAVIES
For those in the West, hunger is often just the familiar feeling of a growling stomach between meals — in Gaza, it has become a strategic weapon of slow, systematic and deadly destruction, writes MARC VANDEPITTE
After almost two decades of rule by the Movement Toward Socialism, once led by Evo Morales, right-wing parties have emerged in the lead after the first round of elections on August 17 and are now in control of the legislature, reports PABLO MERIGUET
DAVID MATTHEWS looks at what a collective future for welfare might have in store for us






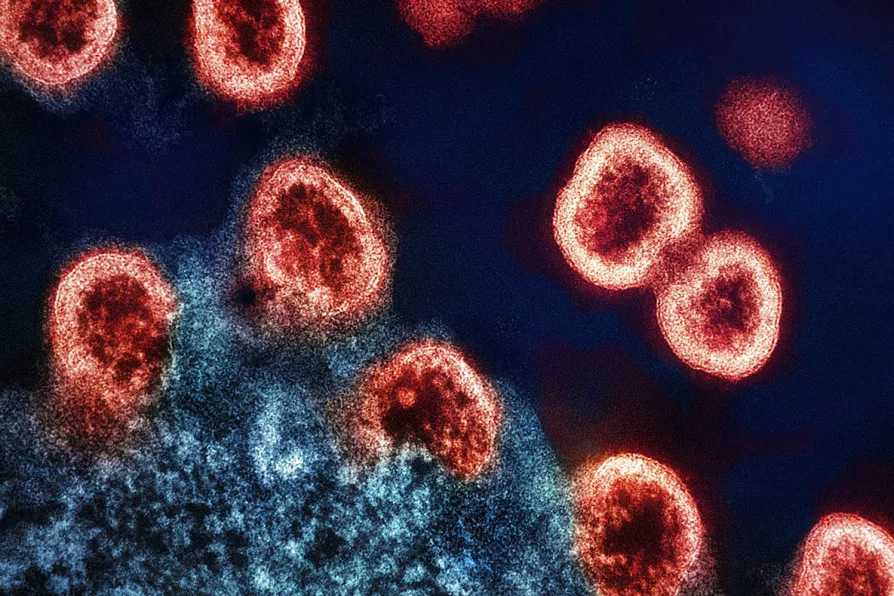
LENACAPAVIR, an injectable antiretroviral drug developed by Gilead Sciences, recently made headlines after a Phase 3 clinical trial in South Africa and Uganda showed it to be 100 per cent effective in preventing HIV among women and adolescent girls.
Though hailed as a breakthrough in HIV prevention, lenacapavir serves as a stark reminder of the problems with the pricing of life-saving medicines.
While further data from this study and results from studies involving other populations are needed, lenacapavir could be considered the most durable HIV prevention method to show efficacy among women — a population for who biomedical HIV prevention evidence has been severely limited.

Similar stories

When privatisation is already so deeply embedded in the NHS, we can’t just blindly argue for ‘more funding’ to solve its problems, explain ESTHER GILES, NICO CSERGO, BRIAN GIBBONS and RATHI GUHADASAN

Despite miraculous trial results showing new treatment could halt transmission, corporate greed and patent laws condemn millions to preventable infection and death, write ROX MIDDLETON, LIAM SHAW and MIRIAM GAUNTLETT
Labour’s controversial plan to put the overweight and unemployed on the ‘skinny jab’ Mounjaro should set alarm bells ringing once we look into some of the research into the drug and the company set to supply it, warns CLAUDIA WEBBE

Keep Our NHS Public campaigner GREG DROPKIN dissects how Lord Darzi’s recommendations align with Starmer’s plans for NHS ‘reform,’ warning of creeping privatisation under the guise of modernisation