Internationalism is deeply embedded in socialist theory and practice. Examination illuminates its complexity asserts the Marx Memorial Library and Workers’ School


Let down by ‘care via video call’
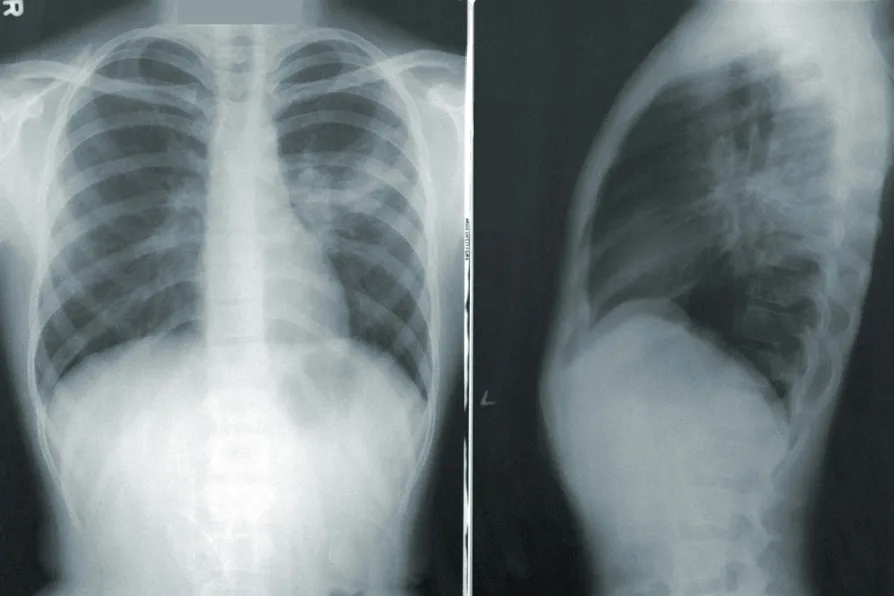
RUTH HUNT looks at the risks of remote appointments for patients with long-term spinal cord injuries, who have substantial clinical needs


The new TUC Cymru general secretary speaks to Morning Star Wales reporter David Nicholson about her trade union background and ambitions for the movement
The Claudia Sheinbaum government is no pushover and is holding firm despite US abuses of the relationship, says DAVID RABY
As we approach the grim anniversaries of Hiroshima and Nagasaki, SIMON BARROW sounds the alarm over the dangerous and murderous direction our government is heading
The new PM may offer more of the same, but early signs on his housing policies look promising, says GLYNN ROBBINS
CLAUDIA WEBBE argues that Burnham’s U-turn on tackling greedy landlords has let the country down






WE know the NHS is going backwards on key performance targets. This raises concern for patient groups, such as those with long-term spinal cord injuries (SCI) who, prior to the pandemic would have a yearly, in-person, monitoring appointment, regardless of their clinical need.
These appointments are crucial because, as those with SCI age, they are more prone to developing life-limiting secondary conditions. But it’s not just physical factors a spinal team should be assessing, as living with a disability or disabilities can also take a heavy toll on mental health.
The NHS Care Pathway for Spinal Cord Injuries calls it: “Lifelong follow-up of people living with SCI to prevent and manage SCI related complications.”

Similar stories

CLAUDIA WEBBE says the horrific price British patients will pay for this NHS deal is now clear — and there’s time to get out of it, if MPs will only force the issue


Seventeen years after losing her council job due to needing endometriosis surgery, Michelle Dewar’s campaign for paid menstrual leave gained 50,000 signatures in a week, reports ELIZABETH SHORT