While international actors discuss governance and reconstruction, Netanyahu has made it clear that Israel has no intention of ending its military occupation, says RAMZY BAROUD

The scourge of restrictive practices in mental health care: ‘It just muted me’
The lack of NHS mental health provision for young people has led to many placements, out of sight and out of mind, in so-called ‘specialist,’ privately run units. This comes at great cost for all involved, writes RUTH HUNT


NICK WRIGHT continues his series analysing the trends in European politics
We have the alternative economics, histories of our struggles and the confidence to change the world
General Federation of Trade Unions assistant general secretary HENRY FOWLER reports on the final day from the GFTU’s residential Summer School at the Workers’ Retreat, Quorn Grange Hotel
Capitalism has exploited — and polluted — our natural resources for too long, it’s time we treated our rivers as living beings, writes MIRIUM GAUNTLETT, LIAM SHAW and ROX MIDDLETON
Treating the Clacton by-election as a joke risks reinforcing the Reform leader’s claim to be the victim of an out-of-touch Establishment, argues JOHN McINALLY
MPs and others called for the urgent release of tortured Palestinian doctor, Hussam Abu Safiya, held hostage by Israel and reportedly near death, reports LINDA PENTZ GUNTER






ALTHOUGH the NHS hands over vast sums to independent mental health service providers, those who have lost loved ones or have been damaged by long periods of restrictive practices, often have to fight to be even acknowledged — let alone get real justice.
For those who have been in these units either as patients or staff, there’s a feeling of relief they have survived. But they also have a need to share their stories, to add further weight to the call to shut these expensive units down and end unsafe restrictive practices.
Steph had a dream of working in mental health, using her own personal experiences and in turn, helping those who are going through similar turmoil.

Similar stories

Gisele Pelicot said ‘shame must change sides.’ We may think we agree, but, argues LOUISE RAW, society still has some way to go
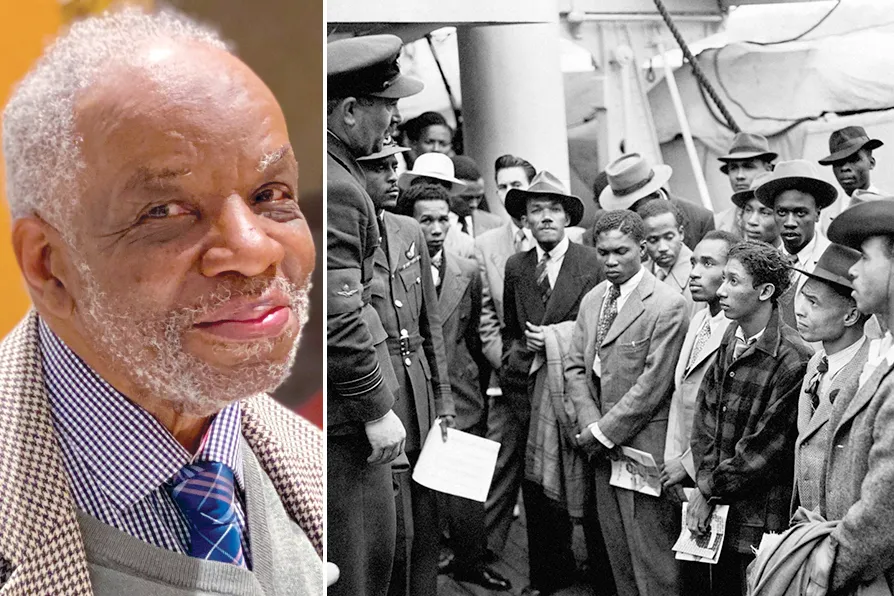
1943-2025: How one man’s unfinished work reveals the lethal lie of ‘colour-blind’ medicine
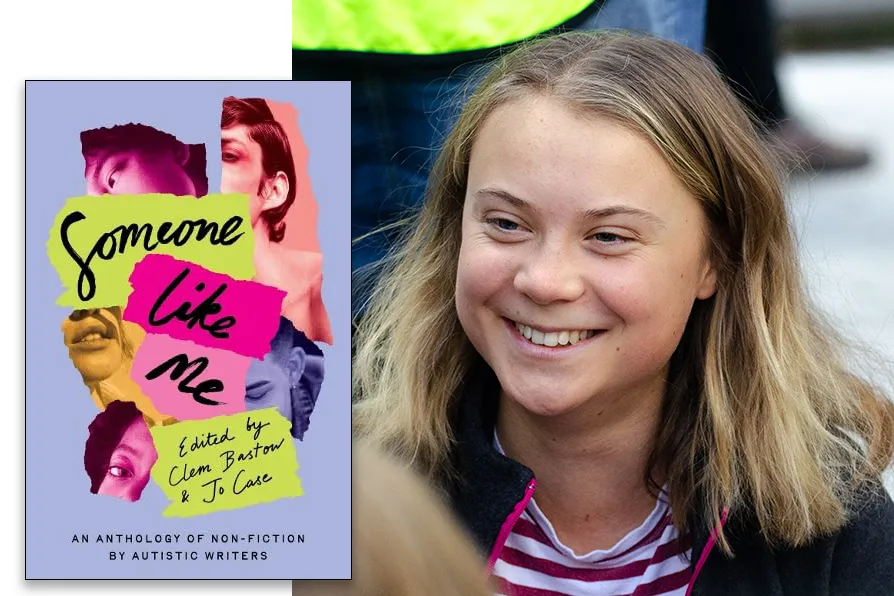
JOSEPHINE BARBARO welcomes a diverse anthology of experiences by autistic women that amounts to a resounding chorus, demanding to be heard

Seventeen years after losing her council job due to needing endometriosis surgery, Michelle Dewar’s campaign for paid menstrual leave gained 50,000 signatures in a week, reports ELIZABETH SHORT