A new generation of right-wing politicians have shifted from promoting deregulation to championing anti-migrant politics warns SOLOMON HUGHES


Lives are being put at risk through the downskilling of the NHS
The government’s latest cost-cutting NHS manoeuvres are a risk to patient safety – they must be vigorously opposed, warns CLAUDIA WEBBE MP

by the Greater Manchester Workers’ and Tenants’ Association
The US relationship with Israel has evolved into a strategic liability, argues RAMZY BAROUD
A champion motorcyclist, trade union organiser and communist, Clem Beckett went from Britain’s speedway tracks to the battlefields of Spain, where he gave his life resisting Franco’s forces at Jarama. GEOFF BOTTOMS pays tribute to this remarkable anti-fascist
The greatest threat to democracy may no longer come from political parties but from unelected tech oligarchs like Peter Thiel and his powerful Silicon Valley network, argues JOHN GREEN
Claiming to ease a fertiliser shortage, the Trump administration has suspended tariffs on Moroccan phosphate imports – deepening US support for the Morocco’s control over Sahrawi territory, writes LUKE ROTELLO






THE British government is preparing to legislate for new “regulated” medical roles in the NHS that it claims will “improve patient safety”: “medical associates.” However, the government and the NHS admit that these roles are not qualified doctors and that they form a key part of the government’s “long-term plan” to increase the NHS workforce.
The new plan for these semi-qualified roles to be regulated by the General Medical Council will drive the supposedly “safe” “expansion of medical associate roles to support doctors and GPs,” amounting to a padding out of NHS numbers to allow costs to be driven down through a “downskilling” of the NHS workforce.
The absence of proper workforce planning since the Conservatives entered government in 2010 was highlighted by the King’s Fund earlier this year as a major cause of the struggles of the NHS, yet the Tories’ response to that now is to fill positions with people who are not as qualified as those the NHS has lost.

Similar stories

CLAUDIA WEBBE says the horrific price British patients will pay for this NHS deal is now clear — and there’s time to get out of it, if MPs will only force the issue


In the second part of her critique of Wes Streeting’s TenYear Plan for Health, HELEN MERCER looks at the central planks of this privatisation blueprint
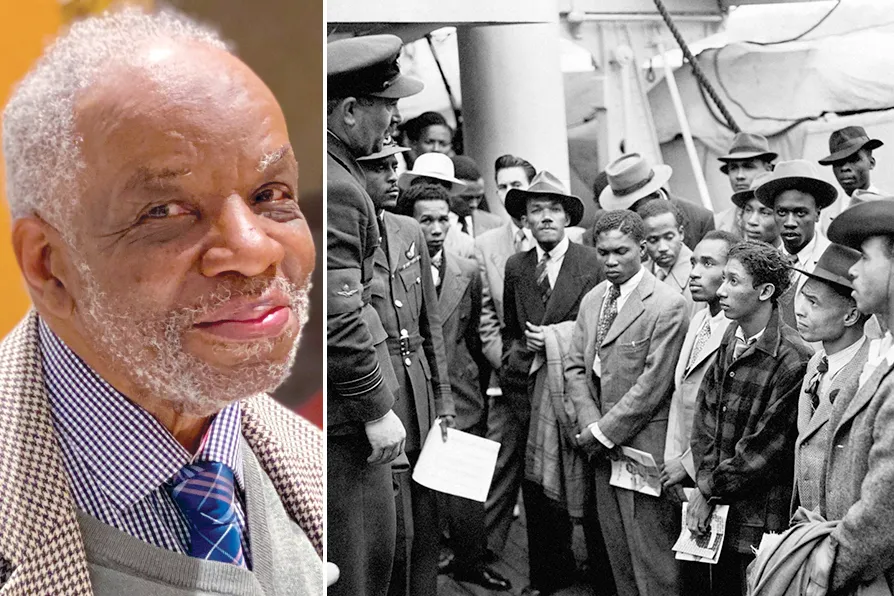
1943-2025: How one man’s unfinished work reveals the lethal lie of ‘colour-blind’ medicine